Suggested readings from Langman's Medical Embryology (13th. ed.):
Ch 15, pp. 225-249
Suggested readings from Langman's Medical Embryology (12th. ed.):
Ch 15, pp. 208-231
Suggested readings from Langman's Medical Embryology (11th. ed.):
Ch. 14, pp. 209-233
I. Overview
A. Formation of the primitive gut tube
The gut tube is formed from endoderm lining the yolk sac which is enveloped by the developing coelom as the result of cranial and caudal folding.
During folding, somatic mesoderm is applied to the body wall to give rise to the parietal peritoneum. Visceral (or splanchnic) mesoderm is wraps around the gut tube to form the mesenteries that suspend the gut tube within the body cavity. The mesoderm immediately associated with the endodermal tube also contributes to most of the wall of the gut tube. Nerves and neurons found in the wall are derived from neural crest.
Summary of germ layer contributions:
endoderm: mucosal epithelium, mucosal glands, and submucosal glands of the GI tract.
mesoderm: lamina propria, muscularis mucosae, submucosal connective tissue and blood vessels, muscularis externa, and adventitia/serosa
neural crest: neurons and nerves of the submucosal and myenteric plexes
B. Basic subdivisions of the gut tube
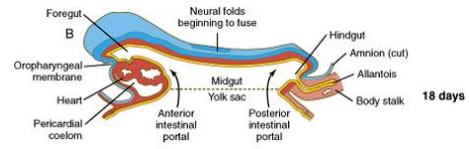
Cranio-caudal and lateral folding cause the opening of the gut tube to the yolk sac to draw closed (like a pursestring) forming a pocket toward the head end of the embryo called the "anterior (or cranial) intestinal portal" and a "posterior (or caudal) intestinal portal" toward the tail of the embryo. These are the future foregut and hindgut, respectively. The midgut remains open to the yolk sac.
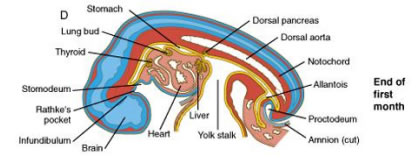
Further folding and growth of the embryo causes the communication of the gut with the yolk sac to continue to get smaller and the regions of the gut (foregut, midgut, and hindgut) to become further refined:
The derivatives of the gut regions are as follows:
FOREGUT
MIDGUT
HINDGUT
Trachea & respiratory tract
Lower duodenum**
Distal 1/3 of transverse colon
Lungs
Jejunum
Descending colon
Esophagus
Ileum
Sigmoid colon
Stomach
Cecum
Rectum
Liver
Appendix
Upper anal canal
Gallbladder & bile ducts
Ascending colon
Urogenital sinus
Pancreas (dorsal & ventral)
Proximal 2/3 of transverse colon
Upper duodenum*
*portion served by ant. & post. superior pancreaticoduodenal arteries
**portion served by ant. & post. inferior pancreaticoduodenal arteries
C. Definitive subdivisions of the gut tube
Within the abdominal cavity, the gut is definitively divided into foregut, midgut, and hindgut BASED ON THE ARTERIAL SUPPLY:
Foregut derivatives in the abdomen are supplied by branches of the celiac artery
Midgut derivatives are supplied by branches of the superior mesenteric artery
Hindgut derivatives are supplied by branches of the inferior mesenteric artery
D. Cranio-caudal patterning of the gut tube
specific regions of the gut tube (i.e. that which will become lung vs. that which become esophagus vs. stomach, etc.) and important junctions (e.g. gastro-esophageal junction) are established by a cranial to caudal pattern of segmental, combinatorial "codes" of HOX gene expression in the endoderm and mesoderm of the early embryo.
E. Radial patterning of the gut tube
concentric layering of the gut tube is accomplished largely via expression of Sonic Hedgehog (SHH) in the endoderm which inhibits smooth muscle and neuronal differentiation close to the endoderm. Farther away from the endoderm, the SHH concentration is lower, thus permitting smooth muscle and neuronal differentiation in the muscularis externa. Later in development, the SHH expression goes away, allowing development of smooth muscle in the muscularis mucosae and neurons of the submucosal plexus.
As the gut tube tube develops, the endoderm proliferates rapidly and actually temporarily OCCLUDES the lumen of the tube around the 5th week. Growth and expansion of mesoderm components in the wall coupled with apoptosis of some of the endoderm at around the 7th week causes re-canalization of the tube such that by the 9th week, the lumen is open again.
This occlusion and re-canalization process occurs THROUGHOUT the tube (esophagus to anus) and errors in this process can occur in anywhere along the tube resulting in stenosis (narrowing of the lumen or even outright occlusion) in that region.
F. Mesenteries of the gut tube (refer to the figure on the previous page)
the thoracic esophagus and anus are anchored within the body wall and are therefore retroperitoneal
the stomach and liver are suspended in a mesentery that is attached to the dorsal AND ventral body walls:
the dorsal mesentery of the stomach becomes the greater omentum
the ventral mesentery of the liver becomes the falciform ligament
the mesentery between the stomach and liver becomes the lesser omentum
the rest of the GI tract is suspended by a dorsal mesentery, named according to the organ to which it is attached (mesoduodenum, mesoappendix, mesocolon, etc.)
some portions of the GI tract remain intraperitoneal in the adult and are therefore suspended by a mesentery.
some portions of the GI tract, however, are applied against the body wall during development and the dorsal mesentery becomes incorporated into the body wall, making the organ secondarily retroperitoneal.
A summary of what is retroperitoneal, intraperitoneal, or secondarily retroperitoneal in the adult:
Retroperitoneal
Intraperitoneal
Secondarily retroperitoneal
thoracic esophagus
abdominal esophagus
pancreas
rectum
spleen
duodenum
anus
stomach
ascending colon
liver & gallbladder
descending colon
jejunum & ileum
cecum & appendix
sigmoid colon
II. Derivatives of the foregut:
A. Esophagus
The region of the foregut just caudal to the pharynx develops two longitudinal ridges called the tracheoesophageal folds that divide the tube ventrally into the trachea (and subsequent lung buds), and dorsally into the esophagus.
As with the rest of the gut tube, the lumen of the esophagus becomes temporarily OCCLUDED around the 5th week of development and recanalizes by around the 9th week.
The esophagus is initially short and must grow in length to "keep up" with the overall growth in length of the embryo.
Clinical considerations
Esophageal atresia
occurs when the tracheoesophageal ridges deviate too far dorsally causing the upper esophagus to end as a closed tube.
usually is accompanied by a tracheoesophageal fistula, in which case gut contents can be aspirated into the lungs after birth causing inflammation (pneumonitis) or even infection (pneumonia).
typically associated with polyhydramnios prenatally (the fetus cannot swallow amniotic fluid and it accumulates in the amniotic cavity). Postnatally, the child will regurgitate IMMEDIATELY upon feeding and, if a tracheoesophageal fistula is present, there will be congestion in the lungs.
Esophageal stenosis
occurs when the esophagus fails to recanalize
also typically associated with polyhydramnios prenatally. Postnatally, the child will regurgitate IMMEDIATELY upon feeding. However, there is usually NOT a tracheoesophageal fistula, so the lungs will usually NOT be congested.
Congenital hiatal hernia
occurs when the esophagus fails to grow adequately in length. As a result, the esophagus is too short and therefore pulls the cardiac stomach into the esophageal hiatus in the diaphragm. The resulting compromised structure of the hiatus can allow other gut contents (usually loops of small bowel) to herniate up into the thoracic cavity.
B. Stomach
appears first as a fusiform dilation of the foregut endoderm which undergoes a 90° rotation such that the left side moves ventrally and the right side moves dorsally (the vagus nerves follow this rotation which is how the left vagus becomes anterior and the right vagus becomes posterior).
differential growth on the left and right sides establishes the greater and lesser curvatures, respectively; cranio-caudal rotation tips the pylorus superiorly
dorsal AND ventral mesenteries of the stomach are retained to become the greater and lesser omenta, respectively
proliferation of mesoderm-derived smooth muscle in the caudal end of the stomach forms the pyloric sphincter (dependent on a variety of genetic factors)
Clinical Considerations
Hypertrophic pyloric stenosis
occurs due to oveproliferation (hypertrophy) of the smooth muscle of the pyloric sphincter
rather common (0.5% to 0.1% of infants), more so in males than females; also tends to run in families
is associated clinically with forceful or "projectile," non-bilious vomiting shortly after feeding (usually ~1 hour) because the hypertrophic sphincter prevents gastric emptying into the duodenum. The vomit is usually non-bilious because the blockage is UPSTREAM of the duodenal papilla where bile is added to the gut tube. The hypertrophied sphincter can sometimes be palpated as a small knot at the right costal margin in the epigastric region –sometimes, contractions of the sphincter can even be seen or felt under the skin.
C. Liver
arises out of ventral foregut endoderm adjacent to the septum transversum (the mesoderm of the septum transversum and developing heart send out signals that induce this region of endoderm to become liver).
the parenchyma of the liver (cords of hepatocytes and branched tubules of bile ducts) intercalates within the tissue of the septum transversum and the plexus of vitelline vessels, accounting for the overall architecture observed in the adult (plates of hepatocytes, which are endoderm derived, surrounded by vascular sinusoids, which are mesoderm derived).
D. Pancreas
the endodermal lining of the foregut forms TWO outgrowths caudal to the forming liver: the ventral pancreatic bud and the dorsal pancreatic bud.
within each bud, the endoderm develops into branched tubules attached to secretory acini (the exocinre pancreas). The endocrine pancreas (islets of Langerhans) arise from stem cells at the duct branch points that then develop into discrete islands of vascularized endocrine tissue within the parenchyma of the exocrine glandular tissue.
Primary rotation of the gut tube (discussed later), causes the ventral and dorsal buds to merge together into what is usually a SINGLE organ in the adult:
the uncinate process of the head of the pancreas is derived from the ventral pancreatic bud
the remaining portion of the head, body, and tail of the pancreas is derived from the dorsal pancreatic bud
Errors in the fusion process can result in an annular pancreas that wraps around the duodenum, which can cause obstruction –the symptoms of which would be similar to pyloric stenosis except that the vomit may be bilious and there would NOT be a palpable knot in the epigastric region.
E. Proximal or upper duodenum
arises from the caudalmost part of the foregut and is served by anterior and posterior branches of the superior pancreaticoduodenal artery, which is a branch of the celiac artery.
with rotation of the gut tube, the duodenum and pancreas are pushed up against the body wall and become secondarily retroperitoneal.
III. Derviatives of the midgut
A. Distal or lower duodenum
arises from the cranialmost portion of the midgut and is served by anterior and posterior branches of the inferior pancreaticoduodenal artery, which is a branch of the superior mesentery artery.
as with the rest of the duodenum, becomes secondarily retroperitoneal
as with the rest of the entire GI tract, the lumen is obliterated transiently during development and then re-canalizes.
Failure to recanalize the duodenum can result in stenosis (narrowing) or atresia (complete blockage), the symptoms of which would be bilious projectile vomiting an hour or so after feeding.
B. Jejunum, ileum, cecum, appendix, ascending colon, and proximal 2/3 of transverse colon
elongates rapidly beyond the capacity of the embronic abdominal cavity and thus forms a U-shaped loop that herniates into the umbilicus and is oriented parallel to axis of the embryo such that there is an upper, or cranial, loop and a lower, or caudal, loop.
the upper loop contains what will be jejunum and upper part of the ileum.
the lower, or caudal loop, contains what will be the lower ileum, cecum, appendix, ascending colon and proximal 2/23 of the transverse colon. The appendix can be seen as a diverticulum that is initially pointed downward or toward the tail.
the midpoint of the loop (which is future ileum) is attached to an elongated remnant of the yolk sac called the vitelline duct that normally becomes obliterated.
Failure to obliterate the vitelline duct can result in diverticula (out pouching of the gut tube) called Meckel's diverticula,vitelline cysts or vitelline fistulas (a connection of the small intestine to the skin). These will often be attached at one end to the umbilicus and at the other end to the ileum.
the gut tube undergoes a PRIMARY rotation of 90 degrees counterclockwise (if you were looking at the embryo) such that the lower loop (which has the appendix) is on the embryo's left side.
as the embryo grows the abdominal cavity expands thus drawing the gut tube back into the abdomen, during which time the gut tube further rotates another 180 degrees such that the appendix ends up in the upper right quadrant.
growth of colon pushes the appendix down to its final location in the lower right quadrant.
Failure to pull all of the gut contents back into the abdominal cavity or to completely close off the ventral body wall at the umbilicus can result in an oomphalocoele, where the gut contents herniate out of the body wall.
Defects and variations in rotation can cause a variety of aberrant anatomical positions of the viscera that are often asymptomatic, but important to appreciate when trying to diagnose and/or treat gastrointestinal problems (e.g. abnormal positioning of the appendix due to malrotation should be considered when trying to diagnose appendicitis). Malrotation can also cause twisting or volvulus of the gut tube resulting in stenosis and/or ischemia.
III. Derivatives of the hindgut
include the distal 1/3 of the transverse colon, descending colon, sigmoid colon, rectum, and upper anal canal.
terminal end of the hindgut ends in an endoderm-lined pouch called the cloaca, which is in common with the developing lower urogenital tract.
the formation of a urorectal septum divides the cloaca ventrally into urogenital sinus and dorsally into the rectoanal canal:
urogenital sinus contributes to the lower urogenital tract:
bladder (except trigone), urethra, and vagina in the female
bladder (except trigone), prostate gland, and prostatic and membranous urethras in the male
rectoanal canal: forms the rectum and upper anal canal
urorectal septum: develops into the perineal body
The portion of the cloaca where the hindgut endoderm is up against the ectoderm of the skin breaks down to allow the formation of the anus.
Failure of the cloacal membrane to break down can result in an imperforate anus.
Failure to generate enough mesoderm during gastrulation can result in anal atresia in which there is insufficient development of the wall (namely the smooth muscle and connective tissue) of the rectoanal canal Failures in the division of the cloaca (usually accompanied by anal atresia) can lead to a variety of aberrant connections of the rectal canal to portions of the urogenital tract.
innervation of the hindgut is achieved via the migration of vagal and sacral neural crest cells into the wall of the hindgut followed by their differentiation into neurons of the submucosal and myenteric plexuses (the same is true for the midgut and foregut except that they receive only vagal neural crest).
Failure of neural crest cells to migrate and/or differentiate into neurons in a portion of gut will result in an aganglionic segment (missing submucosal and myenteric ganglia). The main function of these ganglia is to allow local relaxation in the wall of the gut tube, so the aganglionic segment is tonically contracted, leading to obstruction. For a variety of reasons, the distal portions of the colon are most susceptible to this problem, leading to a condition known as Hirschsprung disease or congenital megacolon. The affected individuals often present with a very distended abdomen due to the presence of an aganglionic segment of colon (usually in the sigmoid colon) that causes a blockage and then backup of feces (and massive enlargement) in the descending colon.
Practice Questions
1. Which of the following is NOT derived at least in part from the midgut?
For items 8 – 10 below, select the one lettered option from the following list that is most closely associated with each numbered item below. Options in the list may be used once, more than once, or not at all.
a. ventral mesentery of the liver
b. dorsal mesentery of liver / ventral mesentery of stomach
c. dorsal mesentery of stomach
e. vitelline duct
f. allantois