| Schedule (w/in Gross Anatomy) | UNSW Embryology (awesome site!) | ||||
|
|
Embryogenesis: fertilization, implantation, gastrulation, somitogenesis |
||
| Suggested readings from Langman's Medical Embryology (11th. ed.): |
|
|
|
|
Practice Questions
Multiple choice/multiple correct. Any, all, or none of the answers to each question may be correct. Please identify all the correct answers. 1. Implantation of human embryos typically occurs:
2. Which of the following is derived from ENDODERM?
3. During the development of the placenta:
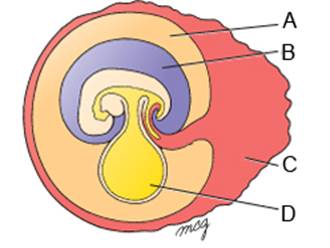
Questions 4-7 refer to the image below. For each of these questions, choose the SINGLE BEST answer.
4. The approximate age of this embryo is:
5. The label indicating the amniotic cavity is:
6. The label indicating a space lined by endoderm is:
7. The label indicating a space containing fluid that is produced by the kidneys in the developing fetus is
Questions 8 and 9 refer to the following case. For each of these questions, choose the SINGLE BEST answer. A 19-year-old pregnant woman at 29 weeks gestation underwent routine prenatal sonography. A large fluid filled, intrauterine structure was found and she subsequently was referred to a tertiary care facility for further evaluation and management. She denied nausea, vomiting, acute abdominal pain, or recent trauma, and her pregnancy had been progressing well. An MRI was obtained to further delineate the lesion found on sonography. MRI showed large cystic mass arising from the sacrococcygeal region of the fetus (Fig. 1). There was no evidence of polyhydramnios. The patient was counseled and monitored until she presented in labor eight weeks later, with contractions every ten minutes, nausea, vomiting, and apparently decreased fetal activity. She was taken urgently to the operating room where a cesarean section was performed and the fetus was delivered without complication. At the time of delivery, the female neonate was noted to have a large, cystic sacrococcygeal mass (Fig. 2) measuring 19.1 cm by 9.7 cm by 13.2 cm. The mass had no solid components, and there was no involvement of the neural tube. The neonate was subsequently taken to surgery where the lesion was resected and coccygectomy was performed. Post-operatively, the mother and child both did well and were discharged home in stable condition. Figure 1. MRI (T2 weighted images) of the maternal pelvis depicting a large cystic mass arising from the sacrococcygeal region of the fetus (the head of the fetus is down). Figure 2. Gross image of the sacrococcygeal mass following cesarean section delivery of the neonate.
8. The MOST LIKELY cause for this congenital defect is:
9. Histologic examination of the mass would reveal derivatives of which germ layer(s)?
|
|
Click here to submit questions or comments about this site. Updated 8/22/22 - Velkey |
||