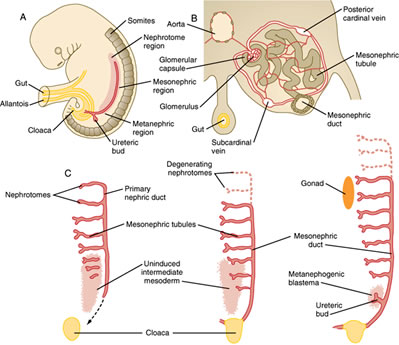
The urogenital system arises from intermediate mesoderm which forms a urogenital ridge on either side of the aorta.
The urogenital ridge develops into three sets of tubular nephric structures (from head to tail): the pronephros, the mesonephros, and the metanephros.
A. The Pronephros
Is the cranialmost set of tubes, which mostly regress
B. The mesonephros
Is located along the midsection of the embryo and develops into mesonephric tubules and the mesonephric duct (Wolffian duct).
These tubules carry out some kidney function at first, but then many of the tubules regress. However, the mesonephric duct persists and opens to the cloaca at the tail of the embryo.
C. The metanephros
Gives rise to the definitive adult kidney.
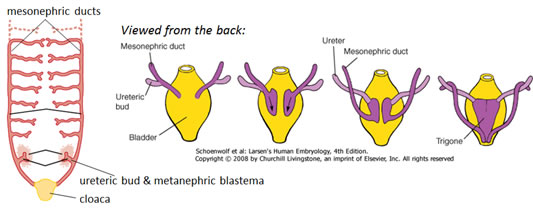
Develops from an outgrowth of the caudal mesonephric duct, the ureteric bud, and from a condensation of nearby renogenic intermediate mesoderm, the metanephric blastema.
II. Steps in renogenesis
Involves a process of reciprocal induction, which is retinoic acid dependent
Cranial-caudal patterning establishes a “renogenic” region within the intermediate mesoderm in the tail of the embryo –this renogenic mesoderm is the METANEPHRIC BLASTEMA
The METANEPHRIC BLASTEMA secretes growth factors that induce growth of the URETERIC BUD from the caudal portion of the mesonephric duct.
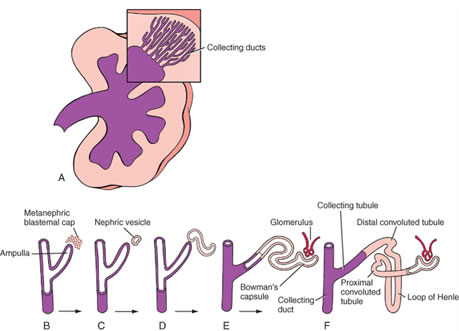
The URETERIC BUD proliferates and responds by secreting growth factors that stimulates proliferation and then differentiation of the metanephric blastema into glomeruli and kidney tubules (i.e. induces the blastema to undergo mesenchymal-to-epithelial transition ).
Perturbations in any aspect of these inductive events (e.g. mutations of either metanephric or ureteric factors or disruption of retinoic acid signaling) may cause inhibition of ureteric bud growth and renal hypoplasia or agenesis. Conversely, duplication or overproliferation of structures can occur if there is a gain of function of the inductive factors.
III. Derivatives of the ureteric bud and metanephric blastema in the adult kidney
A. Derivatives of the metanephric blastema:
Podocytes covering glomerular capillaries
Epithelial cells lining Bowman’s capsule
Proximal convoluted tubules
Descending thick limbs of the loops of Henle
Thin limbs of the loops of Henle
Ascending thick limbs of the loop of Henle
Distal convoluted tubules
B. Derivatives of the ureteric bud:
Collecting tubules and ducts
Minor and major calyces
Ureters
IV. Examples of perturbations in induction or differentiation of kidney tissue
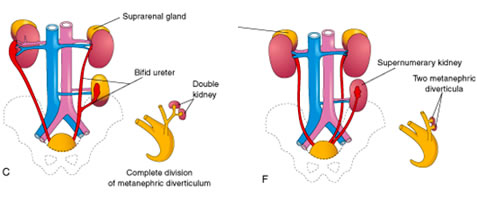
A. Duplication of the urinary tract
Occurs when the ureteric bud prematurely divides before penetrating the metanephric blastema
Results in either a double kidney and/or a duplicated ureter and renal pelvis
B. Renal-Coloboma syndrome
The Pax2 gene essential for metanephric mesenchyme to differentiate into epithelial tubules in response to inductive signals from ureteric bud, so mutations (even if HETEROZYGOUS) can produce renal defects. Patients typically exhibit the following symptoms:
Renal hypoplasia - due to reduced proliferation of the mesenchyme derived epithelia during development.
Vesicouretral Reflux - most likely due to improper connection of the ureter to the bladder or possibly due to inherent defects in epithelial cells of the mature ureter.
Colobomas (ventral fissures in iris, retina, and/or optic nerve) - due to failure of the optic fissure to fuse (expression of Pax2 is observed in ventral part of the optic cup and optic stalk).
C. Nephroblastoma (Wilms Tumor)
found in infants from 0-24 months of age
consists of blastemal, epithelial, and stromal cell types
associated with mutations in genes related to kidney development (PAX2, WT1, etc.)
essentially due to incomplete mesenchymal-to-epithelial transformation (i.e. the cells fail to fully differentiate and transform into cancerous cells).
D. Polycystic kidney disease
can arise due to a variety of factors:
loss of polarity: aberrant differentiation of tubule cells results in inappropriate location of Na/K channels to the apical (rather than basal) domain of the cells. Na+ is pumped apically, water follows resulting in dilation of tubule lumens.
Overproliferation: excessive growth of tubule epithelium can occlude the lumen causing blockage.
A hallmark of renal agenesis, hypoplasia, or dysfunction in utero is oligohydramnios (low amniotic fluid volume) since the amniotic fluid is produced by the kidneys. Reduced amniotic fluid volume causes increased pressure on the developing fetus, resulting in a sloped forehead, “parrot beak” nose, shortened fingers, and hypoplasia of internal organs, particularly the gut and lungs. Collectively, this sequence of anomalies is known as the Potter sequence.
V. Ascent of the kidneys
The kidneys initially form near the tail of the embryo.
Vascular buds from the kidneys grow toward and invade the common iliac arteries.
Growth of the embryo in length causes the kidneys to “ascend” to their final position in the lumbar region.
Rather than “drag” their blood supply with them as they ascend, the kidneys send out new and slightly more cranial branches and then induce the regression of the more caudal branches.
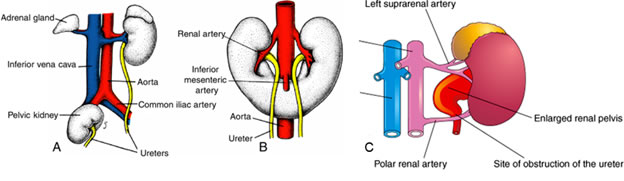
VI. Malformations related to the ascent of the kidneys
Pelvic kidney (A): one or both kidneys stays in the pelvis rather than ascending
Horseshoe kidney (B): the two developing kidneys fuse ventrally into a single, horseshoe shape that gets trapped in the abdomen by the inferior mesenteric artery.
Supernumerary arteries (C): can often have more than one renal artery per kidney, which is often asymptomatic but can sometimes compress the ureter causing a backup of fluid into the renal pelvis and kidney tubules (hydronephrosis)
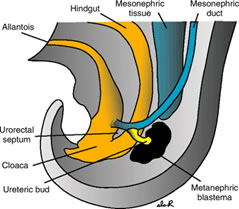
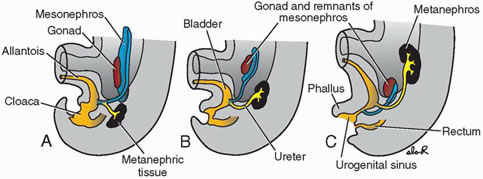
VII. Development of the bladder
The terminal part of the hindgut ends in the CLOACA, which is an endoderm-lined chamber that contacts the surface ectoderm at the cloacal membrane and communicates with the allantois, which is a membranous sac that extends into the umbilicus alongside the vitelline duct.
The cloaca is then divided by the URORECTAL SEPTUM
the DORSAL (inferior) portion develops into the RECTUM and ANAL CANAL
the VENTRAL (superior) portion develops into the BLADDER and UROGENITAL SINUS, which will give rise to the bladder and lower urogenital tracts (prostatic and penile urethrae in males; urethra and lower vagina in females).
As the bladder grows and expands, the distal ends of the mesonephric ducts are absorbed into the wall of the bladder as the TRIGONE.
VIII. Malformations related to the development of the bladder
Trigonitis: As a MESONEPHRIC DUCT derivative, the trigone is sensitive to sex hormones and can undergo hormone-induced epithelial metaplasia (usually transformation from a transitional type to squamous type epithelium which can overproliferate and lead to urinary blockages).
Abnormal attachment of the ureters: the ureters can sometimes be attached to either to the urethra or parts of the reproductive tracts.
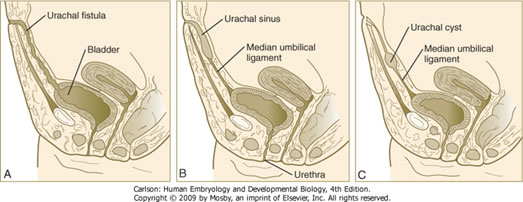
Urachal fistulas, sinuses, and cysts: occur when a remnant of the allantois persists and are found in the midline along the path from the umbilicus to the apex of the bladder (i.e. along the median umbilical ligament).
DEVELOPMENT OF THE SUPRARENAL GLANDS
I. Development of the adrenal cortex
Arises mostly from intermediate mesoderm in the lumbar region of the embryo.
II. Development of the adrenal medulla
Trunk neural crest cells migrate into the center of the adrenal glands and develop into the chromaffin cells of the adrenal medulla. These cells are essentially postganglionic sympathetic neurons that release epinephrine or norepinephrine directly into the bloodstream as opposed to innervating a target organ.
DEVELOPMENT OF THE REPRODUCTIVE SYSTEMS
I. Overview
The gonads arise from intermediate mesoderm within the urogenital ridges of the embryo
The genital ducts arise from paired mesonephric and paramesonephric ducts
The mesonephric ducts give rise to MALE genital ducts
The paramesonephric ducts give rise to FEMALE genital ducts
The gonads and reproductive tracts are indifferent up until 7 weeks of development; differentiation is influenced largely by the presence or absence or SRY (on the Y chromosome)
If SRY+, then development proceeds along the male path
If SRY-, then development proceeds along the female path
II. Development of the MALE reproductive tract
Under the influence of SRY, the gonad develops into a TESTIS containing spermatogonia, Leydig cells, and Sertoli cells.
Leydig cells produce TESTOSTERONE, which support growth of the mesonephric ducts. NOTE: without testosterone, the mesonephric ducts will REGRESS.
Some testosterone is converted into Dihyroxytestosterone (DHT), which supports development of the prostate gland, penis, and scrotum.
Sertoli cells produce ANTI-MÜLLERIAN HORMONE (aka Müllerian Inhibiting Substance, or MIS), which induces regression of the paramesonephric ducts. NOTE: in the absence of MIS, the paramesonephric ducts will PERSIST.
The development of the male goand and upper reproductive tract is shown below - the red tube is the paramesonephric duct which regresses and the purple tube is the mesonephric duct, which develops into the epidydimis and vas deferens:
III. Descent of the testes
The testes arise in the lumbar region but then descend into pelvic cavity and through the inguinal canal to end up in the scrotum
Descent of the testis is due to tethering of the testes to the anterior body wall by the gubernaculum. With growth and elongation of the embryo coupled with shortening of the gubernaculum, the testes are pulled through the body wall, then the inguinal canal, and finally into the scrotum.
IV. Summary of male urogenital tract derivatives
Ureteric bud: ureter
Mesonephric ducts: rete testis, efferent ducts, epididymis, vas deferens, seminal vesicle, trigone of bladder
In the absence of SRY, the gonad develops into an ovary with oogonia and stromal cells.
Since no testosterone is produced, the mesonephric ducts regress.
Since there is also no MIS, the paramesonephric ducts persist to give rise to the oviducts, uterus, and upper 1/3 of the vagina
The urogenital sinus contributes to the formation of the bulbourethral glands and the lower 2/3 of the vagina
The development of the female gonad and upper reproductive tract is shown below - the red tube is the paramesonephric duct which becomes the oviduct and the purple tube is the mesonephric duct, which mostly regresses:
The development of the lower female reproductive tract is shown below - the uterus, cervix, and upper 1/3 of the vagina (derived from paramesonephric ducts) are shown in red and the lower 2/3 of the vagina, bulbourethral glands (purple buds appearing at the end of the movie), and vestibule (derived from urogenital sinus) is shown in yellow:
VI. Summary of female urogenital tract derivatives
Ureteric bud: ureter
Mesonephric ducts: trigone of bladder
Paramesonephric ducts: oviduct, uterus, upper 1/3 of vagina
Proliferation of mesoderm and ectoderm around the cloacal membrane produces primordial tissues of the external genitalia in both sexes: the genital tubercle, genital folds, and genital swellings. The primordia are indistinguishable up until about week 12.
In the MALE, the primordia differentiate as follows:
Genital Tubercle
Genital Folds
Genital Swellings
Body and glans of penis
Ventral aspect of penis
Scrotum
Corpora cavernosum & spongiosum
Penile raphe
Scrotal raphe
In the FEMALE, the primordia differentiate as follows:
Formerly, intersex disorders were subdivided into three main groups as: associated with gonadal dysgenesis, associated with undervirilization of 46,XY individuals, and conditions associated with prenatal virilization of 46,XX subjects. The nomenclature used to describe atypical sexual differentiation has since changed (2,3,4,5). Instead of using the confusing and/or controversial terms such as "intersex," "hermaphroditism" and "sex reversal", the consensus statement recommended a new taxonomy based on the umbrella term, “DSD” (3). This broad category includes common entities such as Turner syndrome and Klinefelter syndrome as well as rare disorders such as cloacal exstrophy and aphallia. Many DSDs are associated with ambiguous genitalia, however, a few may present with delayed puberty or primary amenorrhea.
A. 46,XY DSD - Persistent Müllerian Duct syndrome
Occurs in genetic males with mutations in MIS or the MIS receptor
Because of testosterone and DHT production, there are normal male external genitalia and male genital ducts
Because there is effectively NO Mullerian inhibition, the paramesonephric ducts PERSIST; i.e. there is a small uterus and paired fallopian tubes
The testes may lay either in what would be the normal position for ovaries (i.e. within the broad ligament) or one or both testes may descend into the scrotum.
B. 46,XY DSD - Androgen Insensitivity (aka “Testicular Feminization”) Syndrome
Occurs in genetic males with mutations in the androgen receptor (AR)
Lack of virilization of due to inability of AR to bind testosterone or DHT
XY sex reversal with relatively normal female external genitalia but undescended testes
Mesonephric ducts are rudimentary or lacking due to insentivity to testosterone signaling
Normal production of MIS from Sertoli cells causes Müllerian duct regression, so no oviducts, uterus, or upper 1/3 of vagina
C. 46,XY DSD - 5α-reductase deficiency
Occurs in genetic males with mutations in 5α-reductase necessary for the conversion of testosterone to the more potent androgen, dihydrotestosterone (DHT)
External genitalia are partially virilized
Mesonephric ducts are intact since they only require testosterone (which is still present)
Normal production of MIS from Sertoli cells causes Paramesonephric duct regression
D. 46,XX DSD - masculinized external genitalia due to congenital adrenal hyperplasia
Can present as a DSD in genetic females often due to defects in 21-hydroxylase essential for cortisol synthesis –lack of feedback to pituitary causes overproduction of ACTH and overactivity of the adrenal gland
Increased production of weak androgenic hormones from the adrenal gland (can’t make cortisol or aldosterone but can make androgens such as androstenedione) results in weak virilization of external genitalia:
Enlarged clitoris
Partial or complete fusion of labia majora
Internal genitalia are FEMALE
Testes absent (no SRY)
No mesonephric (male) ducts (no testosterone to support their development)
NO MIS, so the Müllerian (female) duct structures (uterus and oviduct) are intact.
IMPORTANT NOTE: Genetic males (46, XY) can also present with congenital adrenal hyperplasia. However, in these cases, the individuals are already virilized by testosterone produced by the testes, so they would not usually also present with a DSD. However, as their adrenal glands cannot make cortisol and/or aldosterone, they require immediate hormone replacement therapy.
1. The bladder (except the trigone) is derived from tissue associated with the:
For items 14 – 19, select the one lettered option from the following list that is most closely associated with each numbered item below. Options in the list may be used once, more than once, or not at all.
a. metanephric blastema mesenchyme
b. ureteric bud
c. mesonephric duct
d. paramesonephric duct
e. cloaca / urogenital sinus